{kind=link}
{kind=link}

{kind=link}
{kind=link}
{kind=link}
{kind=link}

















Have you been hearing in the news, at school and at work that there are important things you need to do to stay healthy?
BTW, the coronavirus handwashing advice you’ve been hearing about has always been recommended for your healthy daily life!
That’s right, these handwashing basics should be a part of your daily life and your family and friends too! Here’s the Handwashing How!

Check it out — there are 5 easy steps.
This video from the U.S. Centers for Disease Control and Prevention (CDC) gives you all the basics. Share this video with everyone you know.
So now you know how.
Well, there are many times throughout the day, including:
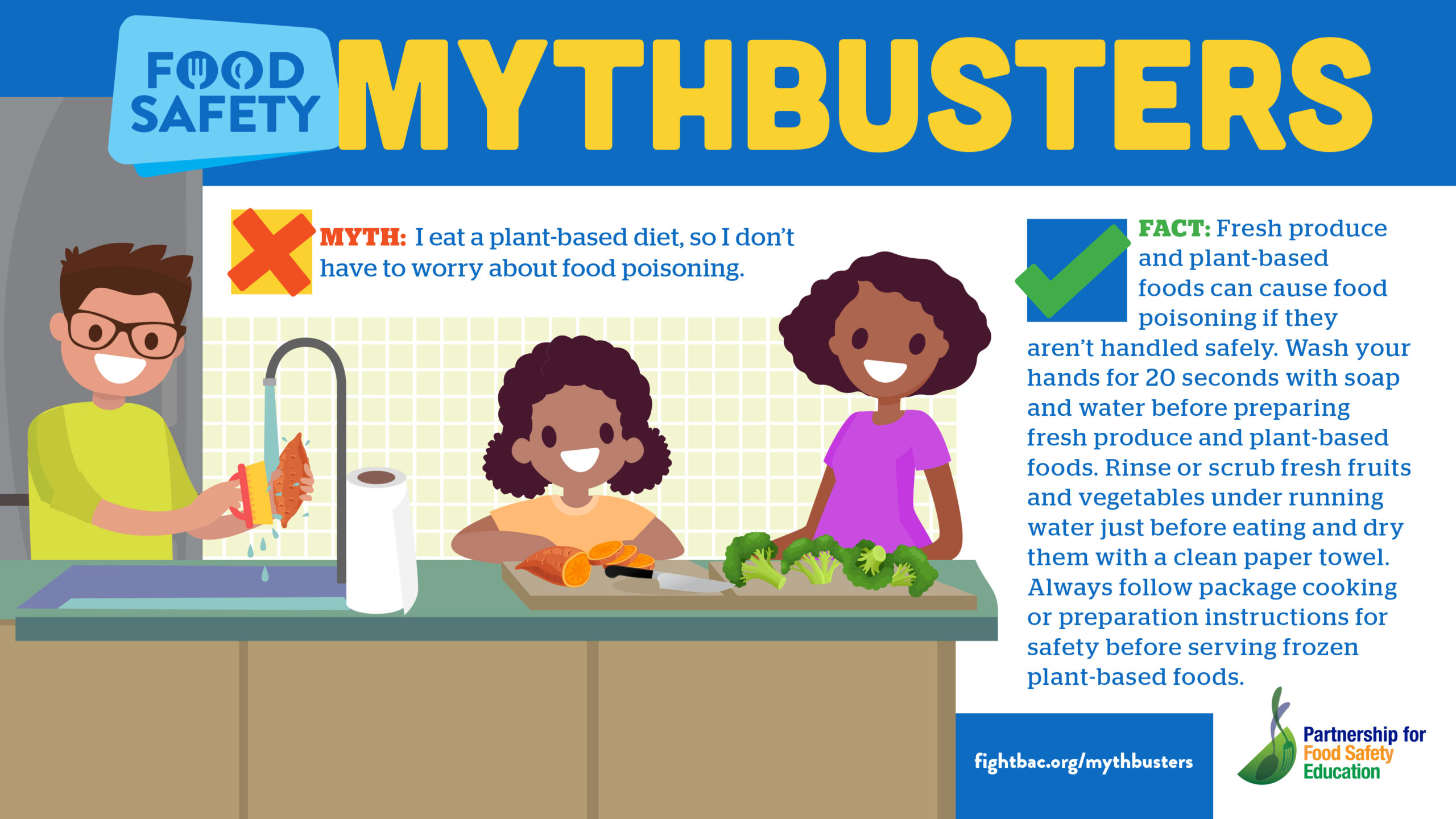
Also, consider that your smartphone or tablet could be a source of contamination. If you use your device in the kitchen while preparing food, you should wash your hands after holding or touching the device.
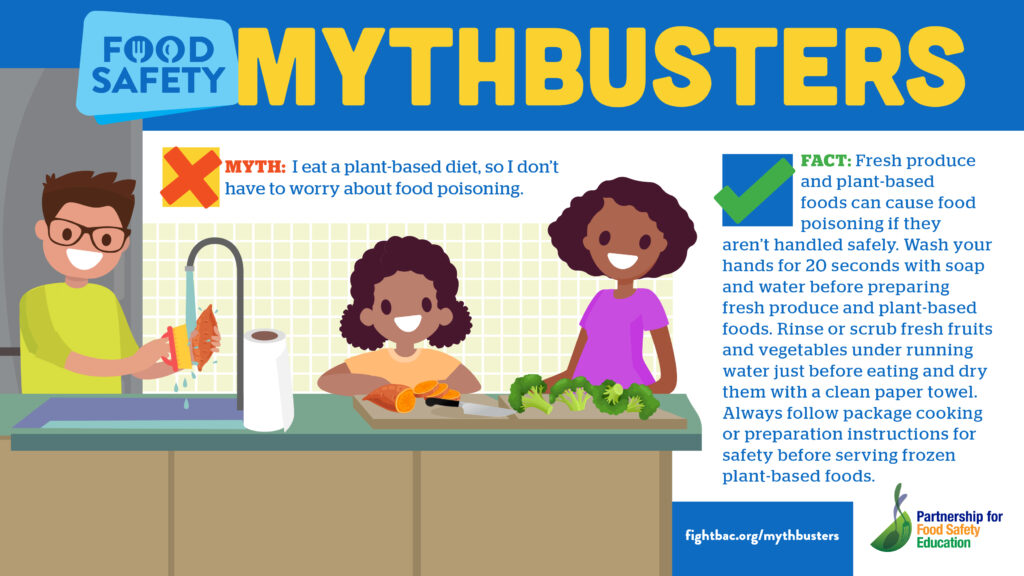
Research shows that “plain” soap is just as good as any other soap. Using soap and water is the best option.
If running water is not available for handwashing, then use a hand sanitizer as a back-up. Your hand sanitizer product should be at least 60% alcohol content in order to be effective.
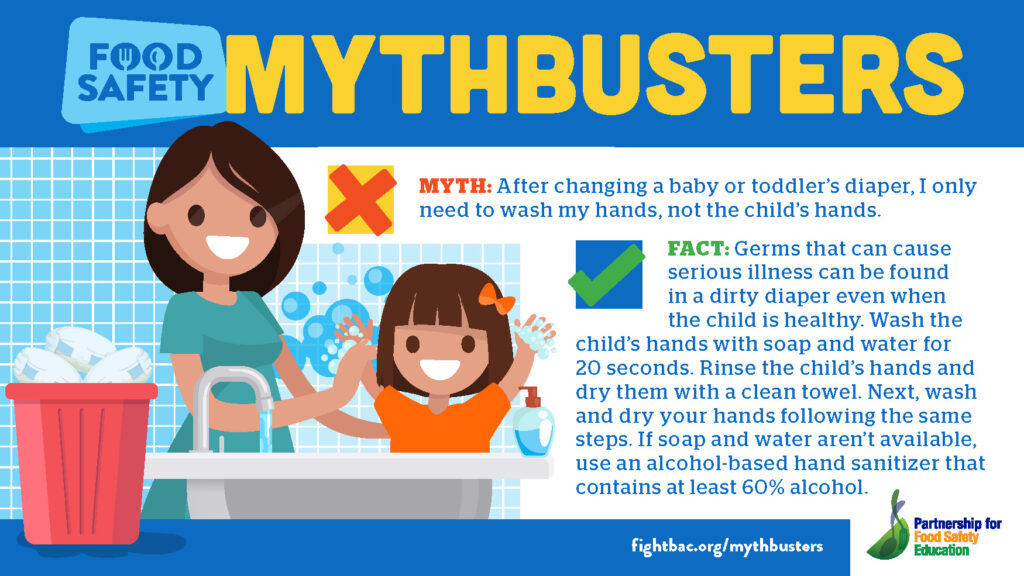
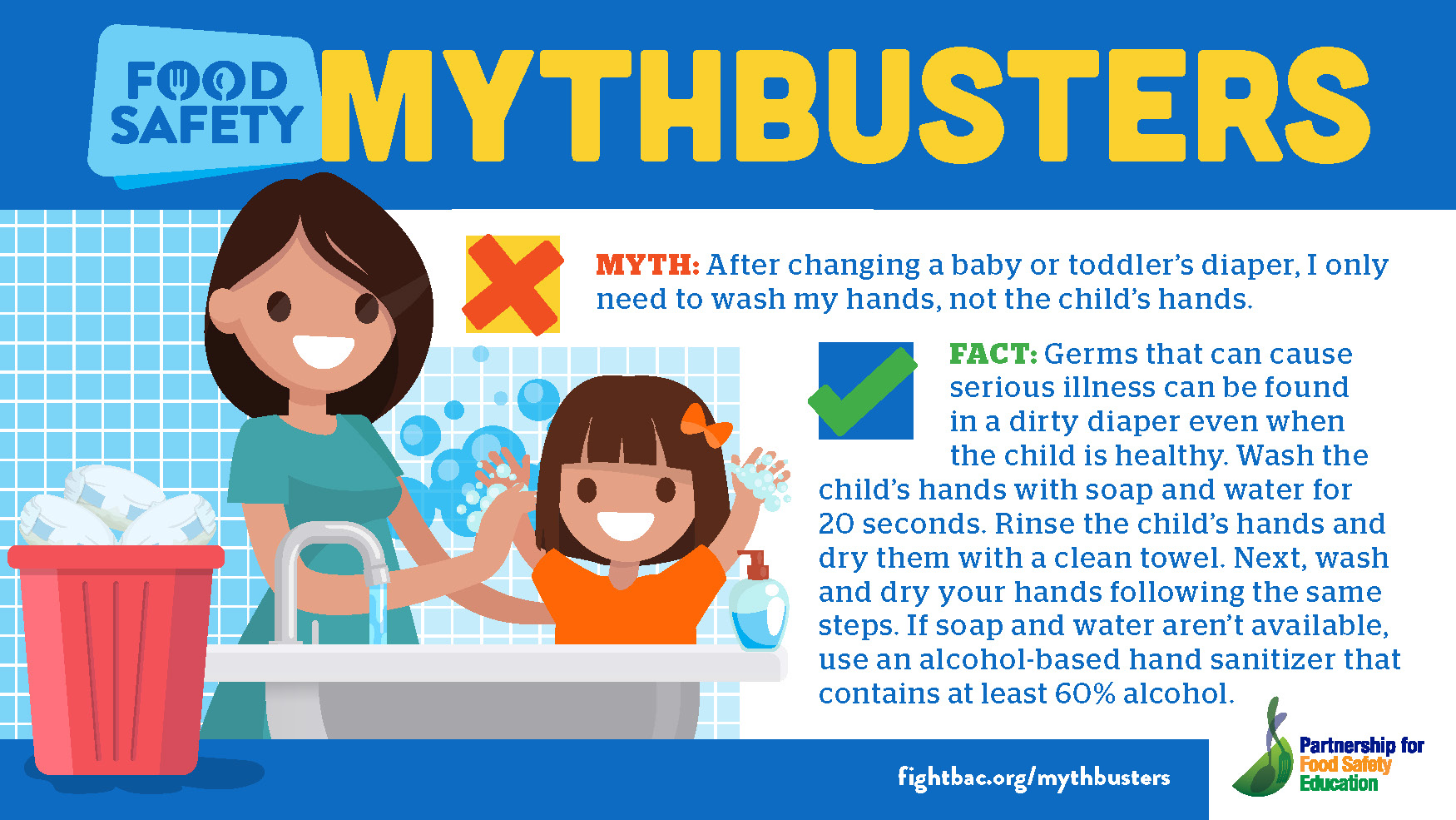
Finally, it is important to take time to help young children wash hands properly.
I know, I know. You’re thinking: I can’t keep up with all the times during the day my child should wash his or her hands.
Still, take time to model proper handwashing. The research about the benefits of regular handwashing says it all. Modeling proper handwashing sets kids up for a healthy life!
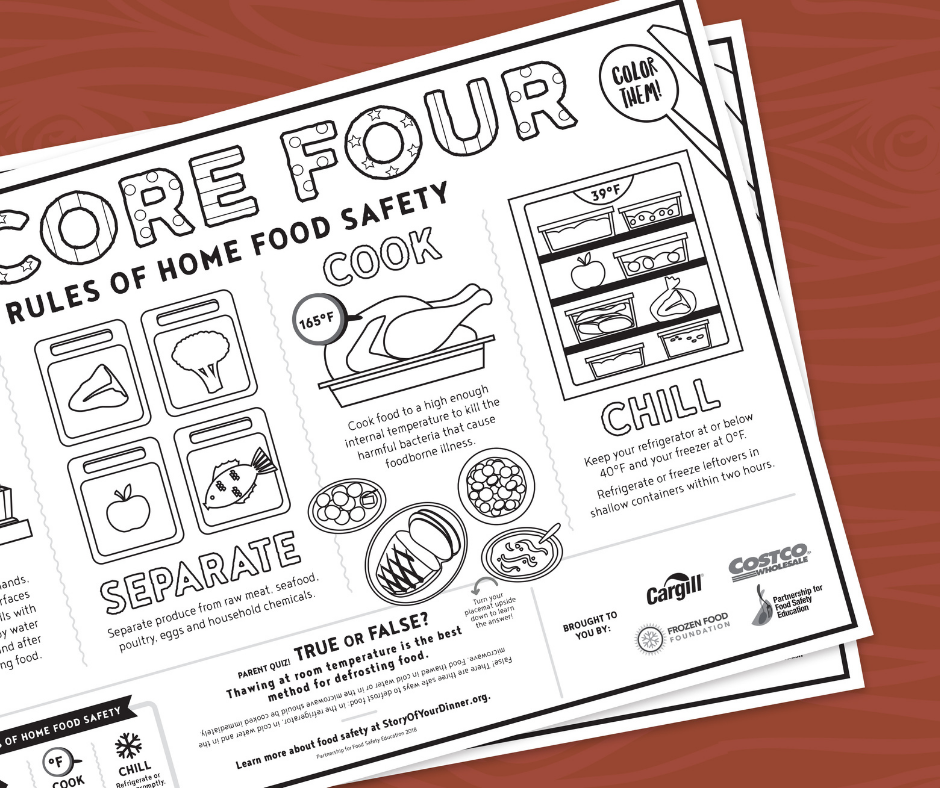
Download a free poster or this Happy Hands song placemat to remind your kids of the 5 steps to proper handwashing!
Happy Handwashing!

Shelley Feist is the Executive Director with the Partnership for Food Safety Education. She can be reached at (202) 220-0651 or sfeist@fightbac.org. Connect: LinkedIn | Twitter








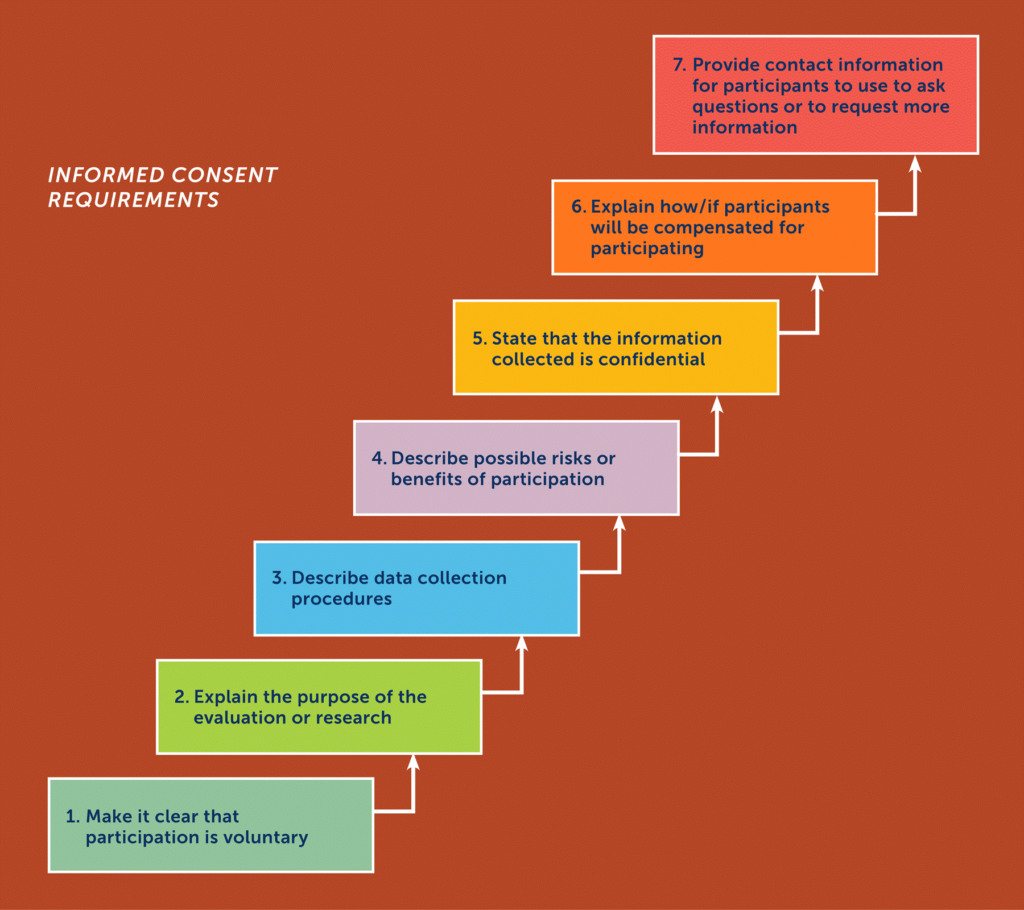
 To evaluate a health education initiative in Georgia elementary schools, pre- and post-test questionnaires were developed to evaluate the program’s effectiveness in increasing knowledge about proper handwashing. Keeping the target audience in mind, evaluation questions were developed to use a similar format to those often used in elementary schools. Extension food safety educators and child development specialists examined evaluation questions for content validity and readability and to ensure they were appropriate for the age- and grade-level of the sample. The University of Georgia Institutional Review Board approved all evaluation methods and instruments. Questionnaires were distributed in test packets students were accustomed to using when taking standardized tests. Evaluation data, collected from 5,462 youth, indicated that the program materials were effective in increasing knowledge about handwashing.
To evaluate a health education initiative in Georgia elementary schools, pre- and post-test questionnaires were developed to evaluate the program’s effectiveness in increasing knowledge about proper handwashing. Keeping the target audience in mind, evaluation questions were developed to use a similar format to those often used in elementary schools. Extension food safety educators and child development specialists examined evaluation questions for content validity and readability and to ensure they were appropriate for the age- and grade-level of the sample. The University of Georgia Institutional Review Board approved all evaluation methods and instruments. Questionnaires were distributed in test packets students were accustomed to using when taking standardized tests. Evaluation data, collected from 5,462 youth, indicated that the program materials were effective in increasing knowledge about handwashing.
Harrison, J. (2012). Teaching children to wash their hands – wash your paws, Georgia! Handwashing education initiative. Food Protection Trends. 32(3), 116-123.